Health Care in Malaysia has evolved significantly in the past 45 years. Prior to the 1980s, in-patient care was mainly in government hospitals. The few non-government hospitals that existed then were run by religious charities on a non-profit basis. However, in the 1980s Dr Mahathir, our Prime Minister then, decided that it would be a good idea if richer patients were given the option of paying for their treatment in private hospitals as that would de-congest government hospitals allowing these hospitals to allocate more of their meagre resources for the poorer patients who could not afford private care.
That policy decision has led to the troubling situation we are in today, where a rapidly expanding private health care sector is exacerbating the brain drain out of the government hospitals. Most specialists hone their skills in government hospitals and when they are sufficiently experienced, leave for the private hospitals, where they can make multiples of their public sector income. This makes it very difficult to build up and maintain specialist units in the government sector as many trainee specialists are enticed out by private hospitals. At present it is estimated that 70% of the specialists with more than 5 years of experience post specialization, are in the private sector.
This maldistribution of specialists between the pubic and the private sectors has led to several problems –
1. There aren’t enough senior specialists in the government sector resulting in long waiting lists in government hospitals, and high workloads for government specialists (increasing the “push” factor inducing these specialists to leave government service).
2. Supervision and training of younger doctors is impaired. There are many talented specialists in the private sector, but they are cut off from the younger doctors in the government hospitals. It is a loss to the profession and the nation, that the way the system has evolved has impeded the transmission of knowledge and skills to subsequent generations of doctors.
3. The expertise of the specialists in the private sector is, on the whole, not used optimally. Most of them were handling the most difficult and challenging cases in the government hospitals where they worked before resigning, but in the private sector they handle the cases that walk into their clinics, the majority of whom could be competently handled by a more junior member of their team in the government hospital.
4. The perceived deterioration of the quality of care in the government hospitals has induced many in the M40 to take health insurance, which is becoming increasingly more expensive. It is an additional financial strain for these families.
However, it should be acknowledged that the growth of private hospitals did benefit the nation in some ways. They probably decreased the out-migration of specialist doctors to other countries. And some of the private hospitals have developed state of the art treatment in various disciplines.
Public-Private Collaboration
Given the current situation where the government hospitals are over-loaded and a significant amount of our health care resources are in the private sector, looking for ways to work together to meet the health needs of our population is a sensible approach. But as the discussion in the section above shows, there can be downsides to policies that give the private sector a larger role in the delivery of health care. We must bear in mind that the development of the private sector can be at the detriment of the public sector and that this disadvantages the poorer sectors of our population, reducing their access to quality care.
To ensure that the collaboration with the Private Sector leads to better health care for ordinary Malaysians, the Health Care Planners must bear in mind the following realities –
- The Private Health Care sector is comprised of 2 large groups. The first group, the private hospitals, are run as businesses and their major shareholders have a much larger say in their management than do the doctors working in them. For Private Hospitals, despite the talk about serving the patients, the public and the nation, the primary aim is to make a tidy profit. The 8000 or so General Practitioners (GPs) are the other somewhat besieged group, pressured by the loss of out-patients to the walk-in specialist clinics in the private hospitals and the strict conditions imposed by Medical Care Organisations and Health Management Organisations. The GPs are an endangered species within the health care system!
- The interaction between the private and the public sector isn’t analogous to the collision of billiard balls. That sort of interaction leaves both parties unaltered by the interaction. Instead, the interaction between the private and the public health care sectors has an impact on the internal organization of both sectors. The section above detailing how the growth of the private sector led to the brain-drain and the weakening of the public sector should be borne in mind.
- There are currently programs where public sector patients are sent out to private centres for certain investigations such as MRIs, and treatments such as angiograms, by-pass surgery and radiotherapy at pre-negotiated rates that are fully paid for by the government. This program is necessary at this point in time as the Public Sector cannot cope with the patient load. But there are some caveats
- This modality of working together can actually accelerate the brain-drain. The increased in workload arising from this referral system, might lead to private hospitals enticing even more government specialists to resign from government and work in the private sector.
- The Public Sector can only negotiate a reasonable price for this form of referrals if the Public Sector maintains (and builds) the capacity to provide the same modalities of treatment. For only then can it refuse to continue the program if the private hospitals hike up prices unreasonably.
So, these sort of programs to off-load the Public Sector have to be seen as a temporary measure to give time to the Public Sector to build up its capacity.
- The MOH must have a strict audit and oversight committee that monitors the agreements for these interactions to ensure that the MOH gets a reasonable deal, and to discourage any tendency of private sector hospitals to influence the public sector negotiation team.
- The Covid vaccination and the PEKA B40 schemes are 2 programs that involved the General Practitioners (GPs) in the country. These schemes have benefited the Malaysian public and this form of collaboration should be developed. The Peoples’ Health Forum1 has recommended that the MOH runs a pilot project which allocates patients with diabetes mellitus and hypertension to GPs to be followed up regularly, with payments to the GP being made on a capitation basis2. Investigations and medications should be provided or fully paid for by the MOH. The participating GPs would be required to comply with management protocols that specify targets for HbA1c, BMI, regular retinal examinations, screening for hyperlipidemia etc.
The British NHS pays an average of 165 pounds per patient per year to the GPs. This works out to 79 RM per month per patient. The rate paid to Malaysian GPs, if such a capitation scheme were to be implemented here, will have to take into account the lower costs in Malaysia as well as the fact that in the British NHS, the GP is allocated a significant percentage of patients who do not have noncommunicable diseases (NCDs). The actual rate obviously has to be negotiated with the MOH.
- Collaboration can also be in the training of specialists. Consultants from the private sector can be invited to run Clinical Case Presentations and other sessions for trainee doctors. Private consultants can be invited to conduct surgeries for difficult cases to enable young specialists to learn some techniques from them.
Negotiating Public-Private Collaboration from a Position of Strength
The Public Health Care System (MOH) will only be able to negotiate a form of collaboration with private sector actors that is beneficial to the Malaysian Public if the MOH is negotiating from a position of strength – both in terms of funds and in terms of human resources.
A. Funds
Many of the schemes involving the private sector in the management of patients referred by the public sector, require payments to the private sector. For example, if the capitation fee for NCD patients was set at RM 40 per month, the cost of referring 1 million patients with diabetes mellitus to be followed up by GPs will come RM 40 million per month – an annual budget of nearly half a billion ringgit.
At present the Ministry of Health gets the second largest ministerial allocation – RM 46 billion this year or 10.9% of the total government budget for 2025. However, this is only 2.45% of Malaysia’s GDP (of RM 1875 bil), far below the 5% of GDP recommended for middle income countries. We take pride in saying we are at the threshold of becoming a high-income nation, but our health allocation is lagging very far below that in the advanced countries – which ranges between 10% to 11% of GDP, except for the USA, an outlier at 16.9%.
Table One: Health Care Allocations in Selected Countries in 2018
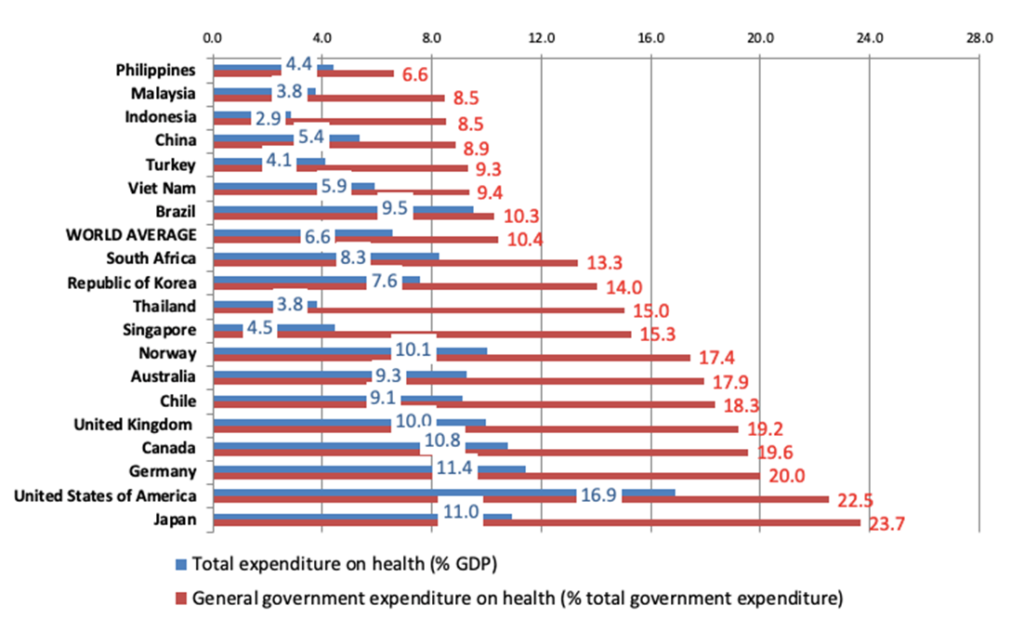
Note – Total expenditure in above table refers to both public sector and private sector health care expenditures.
Source: Global Health Expenditure Database (GHED) 2018, WHO
Whenever the issue of inadequate funding of our public health care system is brought up, the government planners cite the figures similar to those displayed below3, to paint a bleak picture of the nation’s fiscal status, and win our sympathy –
Expected Federal Government Revenue for 2025 = RM 340 bil
Expected Federal Government Expenditure for 2025 = RM 421 bil
Budget Deficit = RM 81 bil (4.3% of the GDP)
Total Federal Government Debt = RM 1,200 billion (64% of the GDP)
Debt Servicing Amount for 2025 = RM 54.7 bil
The Malaysian Government will have to float bonds worth about RM 160 billion in 2025 – RM 81 billion to fund the 2025 budget deficit, and another RM 79 billion to repay the creditors whose bonds are maturing in 2025!
And usually, the discussion ends there. Which is a mistake! The proponents of a larger allocation for health care should master and cite the following arguments –
a) Malaysia is, on the whole, a rich country. Our GDP has multiplied 24 fold4 in real terms in the past 50 years. (Real terms means after accounting for inflation).
b) At this point in time, the ordinary working people in Malaysia receive less than 30% of total national income.
Table Two: Distribution of National Income in Malaysia 2024
Category | Approximate number | Percentage of national income |
Employees – all employees (Government, formal sector, informal sector workers) | 12 mil | 24%a |
Self Employed (Farmers, fishermen, petty traders, gig workers) | 4 mil | 5% |
Owners /Shareholders of Corporations + CEOs, Accountants, Investment Consultants, Senior managers | 0.5 mil | 55%b |
Government | 16% |
c) Meanwhile, the government’s share of national income has shrunk from 30% of Gross Domestic Product (GDP) in the 1980s to 16% currently, making it fiscally impossible to significantly expand the social protection network. The bulk of the wealth created by the labour of our people is appropriated by the richest 3% of individuals and corporations within and outside the country.
d) Corporate tax in Malaysia has been slashed from 40% to 24% of profits over the past 35 years. The government has not as yet started the process of discussing with ASEAN countries to reverse the race to the bottom in corporate tax rates.
The proponents of a stronger social security net for the Malaysian public have to work the above analyses into their arguments. The current maldistribution of wealth was not ordained by the Almighty! It is a societal phenomenon, and therefore, can by society, be re-set. The Global Minimum Tax5 of 15% on the largest multinational corporations is an example of what can be achieved through international consensus.
I am not advocating expropriating all the profits of the largest corporations. But 55% of national income is a bit much! Imagine how the social safety net can be strengthened and climate change mitigated if that 55% that is accruing to the top 3% is reduced to 45%, and an additional 10% of national income is utilized for the social safety net and climate change mitigation. This is what we should aim for in the intermediate term.
B. Personnel
The Ministry of Health cannot negotiate from a position of strength if it continues losing specialist doctors and well-trained nurses and other paramedical personnel to the private sector. The Peoples Health Coalition made the following proposals in its “Blueprint on Health Reform in Malaysia6”.
a. Declare a 10- Year Moratorium on new private hospitals
Every new private hospital draws out a couple of dozen government specialists and a larger number of experienced nurses and other para-medical staff. A temporary moratorium on the building of new private hospitals, would reduce this “pull” factor and enable the public sector to replenish its stock of specialists.
This is not an extreme measure since it does not call for the nationalization of the entire private sector. It allows existing private hospitals to continue running and maintaining their services. The moratorium could be relaxed once a better balance in deployment of our specialist doctors is achieved.
b. Introduce a separate Public Health Services Commission to help retain senior specialists
A separate Public Health Services Commission should be set up to handle public health service staff. Currently, the Public Service Department (JPA) controls salary scales and working term conditions for the entire civil service. However, it is difficult for JPA to delink issues affecting any one particular group of civil servants from the overall civil service, let alone a specific subset such as the senior experienced medical personnel, and respond to the causes of dissatisfaction.
An independent Public Health Services Commission would be able to:
i. Set up more transparent processes for transfers and promotional exercises, with fixed terms and clear criteria for promotion.
ii. Incentivize specialists to remain in public service by awarding them 3-month sabbaticals after every 5 years of service to upskill. During this time, they may choose to subspecialize, learn new skills or engage in activities that are not strictly tied to medical service but still support career progression such as research, publishing and teaching.
iii. Improve the salary scale for doctors and nurses using the Institute Jantung Negara pay scheme as a basis.
Concluding comments
1. Public-Private collaboration in health care delivery is indicated at this stage. Some forms of collaboration such as the capitation scheme for NCD patients transferred to GPs for closer follow-up and better quality care should be envisaged as long term programs. Similarly, collaboration for the transmission of clinical acumen and skills to the doctors in training in the public sector should also be a permanent feature in the Public-Private Partnership.
2. The purchasing of investigational modalities and of surgical services should be seen as a short-term measure to off-load over-stressed public sector doctors until the public sector is able to increase the number of in-house specialists to be able to handle the workload.
3. Successful public-private collaboration efforts is dependent on increasing the allocation to MOH significantly – preferably to 5% of GDP. This will require a redistribution of national income in favour of the government.
4. Successful public-private collaboration efforts also requires measures to retain more public sector specialists through enacting a Moratorium on new private hospitals and on setting up a separate Service Commission for Health Personnel.
Dr Jeyakumar Devaraj
Chairperson
Parti Sosialis Malaysia
25/4/2025
Notes
1. Peoples Health Forum is comprised of Agora Society, Citizens Health Initiative, Health Equity Initiatives, Parti Sosialis Malaysia and Third World Network.
2. Capitation basis – the GP is paid a fixed sum per patient every month, irrespective of the number of times that patient comes to consult him/her.
3. Estimated Expenditure for 2025. Ministry of Finance.
4. KDNK pada harga semasa
1970 RM 11,829 juta; 2019 RM 1,513,157 juta
Dept of Statistics: https://www.epu.gov.my/en/spcio-ewconomic-statistics/socio-economic/national-accounts
Inflation calculator
At beginning of 2020, RM 1000 (of 1970 value) = RM 5294.73 (of beginning 2020 value)
Source: https://www.worlddata.info/asia/malaysia/inflation-rates.php
Calculation: 1513.2 div 11.8 div 5.3 = 24.19
5. Global Minimum Tax of 15% on profits for companies with gross revenue of over 750 million Euros. Has been agreed to by the OECD countries.
6. Available at peopleshealthforum.com